

Play what is in front of you!
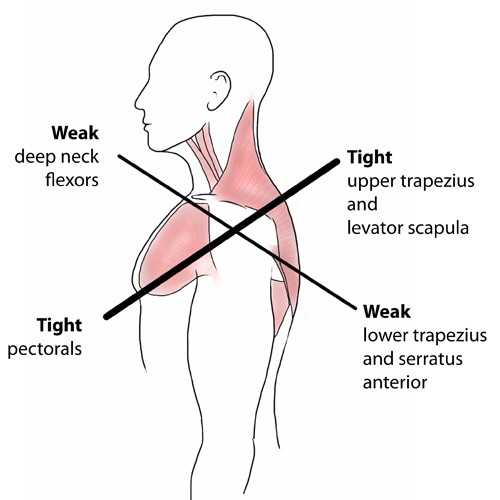
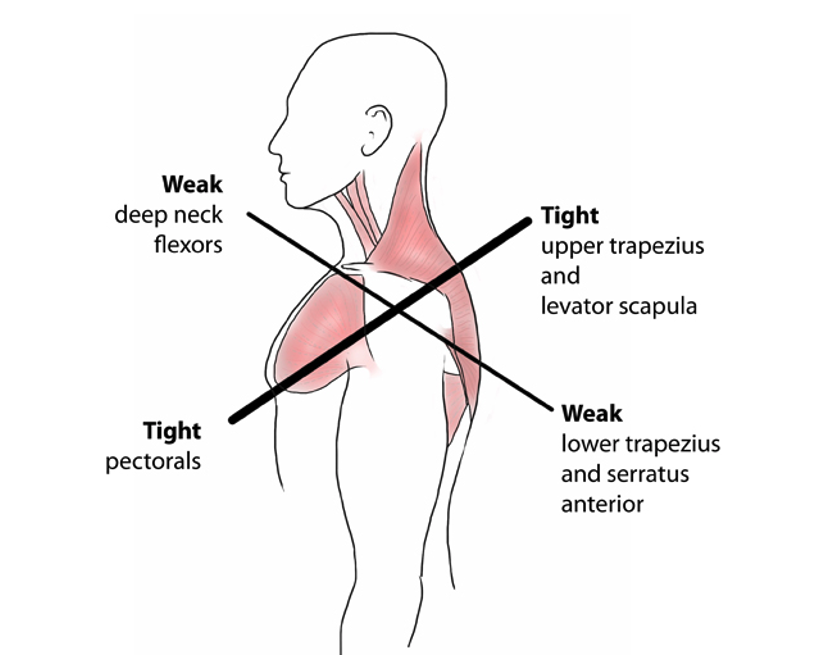
Having played rugby league for nearly 20 years to a reasonable standard and having played a good portion of that in a decision making the role of halfback there are a number of things which have stuck with me, one of the more prominent sayings that were impressed upon us was to ‘play what is in front of you’. What is meant by this is that when you are attacking with ball in hand you need to make the right decision or pick the right pass depending on what the defence is doing in front of you. How does this apply to the clinic? Well if we consider a team who play with a lot of structure to their attack, using all pre-determined plays i.e. we go from A to B to C, the game becomes very cookbook and it is the same with clinic, if a patient presents with X we do Y and Z to get the desired outcome, this works well when we are dealing with a standardised form, however like a opposition defences are unpredictable, patients rarely fit that clearly defined clinical picture which we were taught at university. For example we were taught at university that there was a condition related to posture called upper crossed syndrome (see image), in the 8 or so years that I have been out in the real world I have rarely if ever seen this complete syndrome, have I seen components of it? Yes, was it relevant to the patient’s complaint? Sometimes. Sometimes it needs to be dealt with and others it can be left and the patient will get on just fine leaving it, because to change it would mean altering posture, and posture often comes back to the most energy-efficient and comfortable position for that individual, so we need to play what it is in front of us i.e. the patient and make clinical decisions as to whether something is relevant or not.